Achalasia is a rare oesophageal motility disorder that is often confused with gastroesophageal reflux disease (GERD):
Both conditions can cause chest discomfort, regurgitation and difficulty swallowing, making it challenging for patients to recognise which one they may be experiencing.
However, achalasia and GERD have very different underlying mechanisms and understanding these differences is important for receiving the right diagnosis and care.
This article outlines what achalasia is, how it differs from GERD, how it is diagnosed and when it may be helpful to seek medical assessment.
What is Achalasia?
To understand achalasia, it helps to consider how the oesophagus normally works:
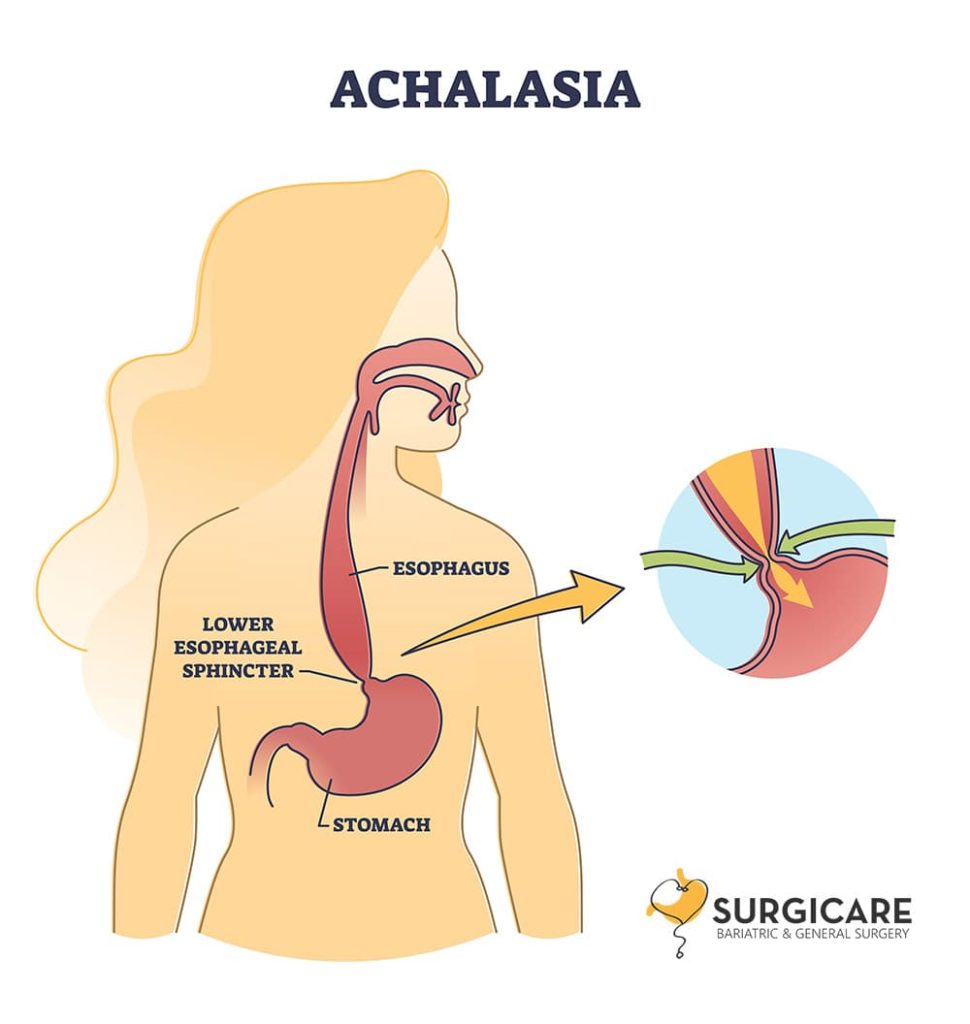
When we swallow, coordinated muscle contractions push food downwards while the lower oesophageal sphincter (LES) relaxes to allow food to enter the stomach.
In achalasia, this process does not function normally. The nerves controlling the oesophagus become damaged or fail to work properly, causing two main problems:
- The LES does not relax adequately
- The oesophagus loses its normal muscular contractions
As a result, food and liquid struggle to move into the stomach, often collecting in the oesophagus. This leads to symptoms such as difficulty swallowing, chest pressure and regurgitation of undigested food.
What is GERD?
GERD occurs when the LES is weak and fails to close properly. This allows stomach acid to flow back into the oesophagus, causing symptoms such as heartburn, acid reflux and regurgitation of acidic fluid (which may leave a sour or bitter taste in the mouth).
Unlike achalasia, GERD is caused by too little closure of the LES, not too much. Despite involving opposite mechanisms, both conditions can produce overlapping symptoms, which is why they are frequently mistaken for each other.
Achalasia vs GERD: Comparison at a glance
| Feature | Achalasia | GERD |
|---|---|---|
| LES Function | Too tight and fails to relax | Weak and fails to close |
| Main Problem | Food cannot enter the stomach | Acid flows into the oesophagus |
| Primary Symptom | Difficulty swallowing (dysphagia) | Heartburn and acid reflux |
| Type of Regurgitation | Undigested food | Acidic or sour fluid |
| Response to Medication | Poor response to acid-reducing drugs | Usually improves with PPIs |
| Progression | Symptoms gradually worsen | Symptoms vary with lifestyle |
Summary
- GERD happens when the LES is too loose, allowing acid to flow back into the oesophagus.
- Achalasia happens when the LES is too tight, making it hard for food to pass into the stomach.
How Achalasia and GERD symptoms overlap, and how they differ
Achalasia and GERD share several symptoms, which is why the two conditions are frequently mistaken for one another.
Both can cause chest discomfort, regurgitation and a sensation of food “coming back up,” especially after meals or when lying down.
However, the type of regurgitation and the pattern of symptoms often differ, offering helpful clues:
In achalasia, difficulty swallowing is usually the main issue. Food may feel stuck in the chest, and patients often regurgitate undigested food hours after eating. Night-time coughing and gradual weight loss may also occur, with symptoms worsening over time.
In GERD, heartburn and acid reflux are more typical. A burning sensation behind the breastbone, a sour or bitter taste, and symptoms triggered by lying down or large meals are common. GERD generally improves with acid-reducing medication, unlike achalasia.
Recognising these differences helps clarify when symptoms may be due to a motility disorder rather than simple reflux.
What causes Achalasia and how it is diagnosed
Achalasia is believed to result from degeneration of the nerves that control the oesophageal muscles.
The exact cause is not fully understood, but research suggests autoimmune or inflammatory processes may play a role. Importantly, achalasia is not caused by acid reflux.
Because achalasia can mimic GERD, diagnosis often requires tests that assess movement rather than appearance alone.
The key investigations include:
- Barium swallow study – shows delayed emptying and narrowing at the LES
- High-resolution oesophageal manometry – the standard test that measures muscle function and confirms achalasia
An endoscopy may also be performed to rule out structural conditions and to assess for food retention in the oesophagus. Some patients undergo pH studies if GERD is also suspected.
Proper diagnosis ensures patients receive treatment that targets the correct underlying mechanism.
Treatment options for Achalasia
Treatment focuses on helping the lower oesophageal sphincter (LES) relax so food can move into the stomach more easily.
While achalasia cannot be reversed, several effective options can significantly improve swallowing and reduce regurgitation:
- Pneumatic balloon dilation stretches the tight LES using a balloon inserted through an endoscope. It can offer good relief, though some patients may need repeat sessions over time.
- Heller myotomy is a surgical procedure that cuts the LES muscle to allow smoother passage of food. It is often combined with a partial fundoplication to help reduce the risk of reflux after surgery.
- POEM (Peroral Endoscopic Myotomy) is a minimally invasive endoscopic technique that cuts the LES from within the oesophageal wall. It is suitable for all types of achalasia and is particularly useful for cases involving oesophageal muscle spasm.
Most patients experience improvement with these treatments. Regular follow-ups help monitor symptoms and long-term outcomes.
When should you seek medical attention?
It may be helpful to seek a medical review if symptoms such as difficulty swallowing, food sticking in the chest or regurgitation persist or worsen over time.
This is especially important when reflux medication does not improve symptoms or when unintentional weight loss occurs:
Although the long-term risk of oesophageal cancer in achalasia is low, persistent or progressive symptoms should still be assessed to ensure the correct diagnosis and appropriate management.

While achalasia and GERD can seem alike, they arise from different problems within the oesophagus and therefore require different approaches to diagnosis and treatment.
If symptoms do not improve with usual reflux measures, a review with a gastrointestinal surgeon can help clarify the cause and guide the next steps.
Call our clinic at +65 6250 5610 or WhatsApp us for an appointment with our specialist.
